Format for use cases, storyboards, activity diagrams and interaction diagrams
return to: Patient Care
further to: Care Plan Glossary
further to: Care Plan Storyboards
further to: Care Plan Use cases
This document is meant to give some guidance in the way we create use cases. It is work underway: tables and figures need to be corrected, chapters and lay out as well.
1. Information analysis for the Electronic Health Record
dr. William Goossen, Results 4 Care, the Netherlands
1. Introduction
In healthcare an enormous amount of patient data is processed. The use of automatic information systems is rapidly growing. The information systems for daily care are called Electronic Health Record’s or EHR’s. The use of EHR’s however is not common everywhere yet. In most healthcare delivery-settings paper records are still common. The patient record, either digital or in paper, is the guide for care professionals throughout the day. When diagnosing or deciding on the necessary care, planning, executing and evaluating care additional information arises. This information is added to the record. In the current paper system, we often see a record for each discipline; a record exists of different components. For the process of care as a whole, these are little islands of information.
In an EHR all the information about a patient is recorded, processed, presented, communicated and archived. Doctors, nurses and allied health professionals (physiotherapist, occupational therapist, social workers, and etcetera) increasingly use an EHR. Within an EHR all information about the patient is gathered, also for future use. The EHR has more advantages, e.g. better readability and exchange-ability of data. All care professionals (on certain conditions) have access and are able to use the EHR. Realization of a nation wide used electronic health record is a process that takes years. In this process progress is made step-by-step. In many instances care professionals will have their own EHR system and might want to exchange information electronically with use of message standards such as Health Level 7.
A condition for working with an electronic health record (EHR) is that it is as serviceable as a paper record. The nurse should be able to specify what information should be included in the EHR and who can benefit from this information. This is because there is a lot of data exchange between different care professionals. When a patient is transferred, for instance from the intensive care unit to a ward, or from the hospital to a nursing home, data should be transferred too. This is the same when a patient goes home when there will be additional care at home.
An information analyst can help the nurse to deliver the accurate data about the care process by asking the right questions. An important step in the development of a national EHR is the execution of the information analysis. The purpose of this paper is to explain the process of information analysis and what products will come out of it.
2. Information analysis of care processes
Information analysis consists of several parts. These are described below.
First part is the identification of the Topic or area of interest: what should the EHR do and for whom? Here the stakeholders are identified and the overall goals for the EHR or project are expressed. For instance: determine a continuity of care record for stroke patients that facilitates in safely exchanging information from general practitioner to hospital to rehabilitation centre to nursing home to home care.
The Second part is the mapping of the care processes to the EHR. Patient care usually takes place in several steps or phases. These can be described separately to attain clarity and to determine what functionality the EHR must have to support these phases. For instance the route a stroke patient typically will follow from being found via Emergency Department to Stroke Unit to follow up care etcetera.
The third part concerns the development of use cases and storyboards. Sometimes these can be similar to clinical paths. Each step or phase from step two is now written out in detail: how does it start, what happens next and what is the end point of a phase. The term ’use case’ is another expression for this step, but refers more to the reason of existence of the storyboard. An example use case is: general practitioner using his PDA when called to a patient. The storyboard around this can be like follows: the general practitioner is called to the home of a patient and assesses that it is stroke and he calls for an ambulance. The EHR on the mobile equipment (PDA) already electronically sends name, address, vital signs and initial diagnoses to the paramedics from the ambulance team. An alternative example of an use case for the EHR: supporting of discharge planning. Example storyboard: after 6 days of admission the stroke patient is stable and the transfer nurse organizes placement in a nursing home. The information analysis will reveal further what needs to be exchanged, what is the trigger to start the discharge process etc.
The fourth part consists of the various communication moments between caregivers. You can think of transfer, a request for a test or handing over responsibility of care for a patient to someone else.
The fifth part is collecting all the information that plays a role in care processes, storyboards, and communication moments. The data that are documented and / or exchanged on different communication moments should be named specifically. There are datasets that are repetitive and there are datasets that are unique for every process. This part of the information analysis leads to an overview of all the data used during the care process. This can be shown, if relevant, in an Excel worksheet. Where available, it is possible to map standardized clinical terminology to each data element.
In some cases, a sixth part of information analysis can be used. When talking about really critical medical decisions, it is sometimes necessary to perform a knowledge analysis. This is beyond the scope of this paper though.
3. Resources for information analysis
To develop an EHR, it is important to narrow down the topic to manageable size and content: the domain of interest. Here any approach can be taken. It is smart to link the topic to existing wording used in the domain to well established keyword systems, such as the UMLS. This is to find additional resources. So the appropriate description of the domain under analysis is important.
Information analysis asks for several resources that are essential to get a complete and correct overview. Live resources are current records and forms, but also literature, health standards, guidelines and protocols may be used. The latter resources most often describe an ideal health care delivery process. This is not always documented in the live records though.
National projects increasingly cause a national basic or core dataset to emerge. Examples are found for CVA-chain healthcare delivery, for youth healthcare delivery and in the near future probably for e-diabetics care. A basic dataset is useful because experts in their professions have thought about the data they wish to be included in the basic dataset.
Health care delivery processes can be observed too. With this we can get a good overview on how care is performed in practice and who is contributing when to this process. It often helps to discuss the observations with care professionals. They will be able to give explanations, come up with alternatives or more details, or other additions. Further, getting feedback also gives clinician’s the option to review their existing work. E.g. for a care situation a dietitian was usually called in for patient’s undergoing cancer therapy. The dietitian was asked to come on day 5. However, when the process was analyses and discussed, the team became aware that the dietitian needs some days to do an assessment and give recommendations for diet. The team changed their process so that the dietitian was called in on day 3. The last step in information analysis is interviewing care professionals. These interviews can be used to verify the overall findings of all 6 steps of the information analysis. This is referred to as verification. Interviews might also give insight into ideas and expectations professionals have for the improvement of data-processing.
4. Processes
In order to analyze health-related information it is important to learn to analyze the departmental or organizational activities objectively. Nurses have several tasks that are performed in a structured manner to present good care to patients. In this way you can also learn to understand the routines the different types of patients get in departments and organizations. By example, care professionals perform a standardized set of actions for the patients with stroke. Some of the activities are the same for all patients, like the support with daily-life-activities, but there are activities that are patient-specific. We can conclude that there is a more or less hierarchical structure in the activities:
1. Department of neurology
2. Stroke -patient
3. List of the problems or disorders of the stroke patient
4. Standard nursing interventions that are carried out for every patient
5. Illness or disorder-specific nursing interventions
6. Individual patient specific list of problems and nursing interventions
The list of all the stroke -patient-related activities of nurses, physicians and physical-therapists can be called the care delivery-process. By describing a care delivery-process you don’t only know what information is needed to give good care, but also by whom and when. Figure 1 illustrates the care delivery-process in a familiar way for care-professionals.
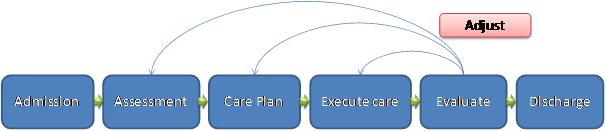

Figure 1. Schematic overview of the care delivery-process from admission to discharge.
5. Storyboard
A storyboard or care-path is a disorder-specific or situation-specific compact description of care needed. It is the basis for information-analysis and information-modeling. Care-path is also referred to as care-scenario or ‘use case’. A care-path is based on the knowledge of care-professionals and research in literature and other resources. A description of a storyboard or care-path contains the following components:
1. the use case: why will this be used by care professionals? What is the purpose?
2. a short description of the case or care-path, which follows a step by step storyboard: e.g., a patient enters the organization with pain or malfunctions and asks for help.
3. He or she is treated by one or more (specialized) care-professionals.
4. Referring to other specialists or departments within the responsibility of the caregiver is part of this stage.
5. Listing of actors (fellow caregivers) in the care delivery-process and their responsibilities when relevant
6. Initial situation or starting point in the care process
7. Listing of activities and interactions (including any communication between sender-receiver)
8. Description of every activity and interaction
9. Aim of the actions and interactions: why is this performed
10. Final situation or end state
The comparison of the care-path with literature is to increase the validity and reliability of the material.
The material is used as resource for the information modeling-process. It is important that de care-path is verified by a care-giver before entering the stage of information-analysis and modeling. The result of this stage is a written description of the desired care-paths. See the example below.
Example: During the 3rd week of her stay in hospital the conclusion of the multi-disciplinary patient meeting is that Mrs. Klaassen’s treatment is finished. A transfer to a nursing home is discussed. This needs to be discussed with mrs. Klaassen and her daughter Jannie before taking other actions. After this is discussed and consent is obtained, the nurse arranges the help of the department for transfers. This employee and the nurse together will collect the information the assessment team needs in order to arrange a quick transfer.
Initial situation / use case: patient can be discharged and information is necessary • Actors: multi-disciplinary meeting, patient, family, nurse, employee of the transfer-department, assessment team, nursing home. • Actions: • Multi-disciplinary meeting concludes to resign the patient • The nurse talks to the patient and family • The nurse arranges the help of the employee transfer • The nurse and the employee transfer make a request for an assessment at the assessment team • The assessment team sends back the results • Final situation: a transfer acceptance for a nursing home is given and the patient is transferred.
The different aspects of the care-path in the example mentioned above are key-elements in the interviews the information analyst has with care-professionals. A study of the forms used in the process of a care-path in addition to the interviews is recommended. These forms can offer structure in the patient-specific information that needs to be collected. Recommended is to use the forms as resources, not as the main input for the digital version of the EHR function to be developed.
6. Communication and interactions
A different way of visualizing information-analysis is by interaction tables. In an interaction table you can register what information you want to exchange and with whom, the aim of the information-exchange and the necessary input. The information exchange takes place between actors or occupational groups, a sender and a receiver. Trigger events are events that start a series of actions.
Designing interaction tables implies clear, logical thinking about the succeeding phases in a care delivery-process. Nurses can deliver the correct information the information-analyst needs to fill the interaction-table with. Cooperation in filling the interaction-table helps both information-analyst and nurse to structure the description of the process. Therefore it is important to limit the width of the different phases to a minimum. This will raise the quality of the interaction tables. This method only increases the transparency of the care delivery-process and also delivers the basis for the specification of the EHR and the electronic messages that are transmitted between the systems. These are the characteristics a message needs when being sent from one to another system. The characteristics are necessary for the receiver to be able to read and understand the message. Table 1 illustrates a part of an interaction table.
Table 1: illustration of a part of an interaction table.
| Sender | Receiver | Purpose | Subject | Data | Current Means | Use of EHR | Result | |
|---|---|---|---|---|---|---|---|---|
| Nurse | Physical-therapist | Apply Therapy | Stroke | Name,indication, date of admission | telephone | Electronic message | Date and time physical therapist gives therapy | |
| Employee transfer point | Assessment Team | Request for transfer Assessment | Problematic situation at home | Necessary admission information | Electronic message | Assessment |
7. Specify and group information
The information used can be deducted from the existing records and forms, observations and interactions. A collection of data with which the table can be filled will emerge. This is how overview is created. Table 2 reflects a schedule in which some of the characteristics of a new-born baby are collected.
Table 2: Data specification fragment from dataset for New-born Item no. characteristic Value 108 Multiple birth Letters: b = boy g = girl (ex. bbg = triplets with 2 boys and 1 girl) 109 Serial number when multiple births 1 = first of the multiple births (time of birth is qualifying) 2 = second of the multiple births 3 = third of the multiple births Etc. range = 1 t/m 8 110 Weight at birth Measured in grams 111 Lowest weight Measured in grams 112 Length at birth Measured in centimeters 113 Girth of skull Measured in centimeters
In information-analysis it is necessary to define the correct level of detail. This is called ‘to granulate’: how specific should the information be? Apart from that it is necessary to group the information. Describe characteristics of information and sort the information into groups. To facilitate this, Detailed Clinical Models (synonyms are care-information models or templates or archetypes) are available. Detailed Clinical Models are based on health informatics standards, terminology and where possible evidence based clinical materials. These are made in several different projects in healthcare. Detailed Clinical Models consist of clusters of information (building blocks) that almost always go together in healthcare.
In the development of the national EHR the Detailed Clinical Models play an important role in maintaining high efficiency of information exchange. Detailed Clinical Models are developed only once and nationally used. Detailed Clinical Models are effective because they provide a standard and they will, on the long term, contribute to the transparency of the effects of care.
Detailed Clinical Models can be seen as an instrument to group knowledge on specific items and to specify the characteristics. In the process of specifying characteristics the unity of the ‘language’ used is increasing. This means international definitions and standards in healthcare arise. Unity of speech is best realized by using an international terminology system. SNOMED CT is available in many countries now to fulfill that function. There are also terminology-systems specifically made for nursing. For some patient groups specific datasets are made including their own terminology. There are several terminologies in use at the moment.
A data-matrix sometimes helps to clarify who needs what information. From this matrix it’s easy to extract the moments that need communication. For every user-communication moment the goal of the interaction is specified in the matrix. As well as the identification of the communicating users, what Health Level 7 interactions and messages can be used and for every interaction and what (sub-)set of data is being exchanged. Table 3 displays an example.
Table 3: simplified data-matrix Interaction Professional 1 Professional 2 Professional 3 Professional 4 Data Blood pressure X X HbA1c X Examination feet X
8. Legislation for communication and registration
Many of the data that is exchanged originates from the patient records. Possible patient records are the medical record, the nursing record, the health record or the paramedical record. The data might for example be collected in the assessment phase, when designing the healthcare delivery-plan or when writing up the documentation. There is a strong connection between the data used for communication and the data used for documentation. This connection is important because when registered, data can be used for multiple purposes. This implies higher efficiency in data-entry per patient. High efficiency is important for the information-analysis. By asking nurses or physicians on pertinent information they need, and to organize this in topics, a correct overview of the necessary data arises. This implies good cooperation within a team consisting of a healthcare professional and an information-analyst. When they manage to complement each other it’s possible to get an end result that suits the desires of the end-user and contributes to EHR development or appropriate message definitions. Documentation is of great importance. Objective documentation is even more important because the data might be used by several different professions in different stages of the care-delivery process. The multiple-use of data produces legislation to be of importance. Legislative demands concern registration and communication. Most countries have laws in place that imply several requirements on care-professionals. One requirement is to maintain a record per patient. The record has several functions .
Maintaining good documentation of the care delivery-process for later use by other care-professionals ; Justification of doings, the record can be used as resource for legal procedures; A means for the patient to have insight in the treatment
In addition to laws, there are usually professional organizations setting guidelines for professional documentation.
9. Unified language
An important requirement is to use standardized terminology when documenting data and referring a patient to a colleague. In the nursing-information system, especially with electronic exchange of nursing information, standardized terminology is important. The receiver or the reader of the information needs to understand easily what the sender or writer has meant with the message. Standardization in the documentation is an important topic in the history of health care. Florence Nightingale is often referred to as one of the founders of professional nursing. In her ‘Notes of Nursing’ (1860) she gives the first outline for classifying and grouping patient-related problems varying from health related items to nursing actions. Nightingale’s work was also a great contribution for modern time healthcare statistics. Classification supplies the necessary standardization and comparability of data and is of vital importance to statistics. Classification is also a means to improve patient-related healthcare (by example by preventing errors) and it is an improvement of the communication and documentation. Documentation is increasingly executed based on multi-disciplinary healthcare delivery-plans. This is where the need comes from to have a multi-disciplinary framework of standardized terminologies at ones proposal.
10. Further stages in the development of EHR after information-analysis
As soon as the data used for care delivery are collected and classified, the next step in analysis can be made. This concerns the modeling of data. We focus on this topic in the next chapter.
Literature • Nightingale, F., 1860. Notes on Nursing. New York: Dover Publications,.
2 MODELING CARE DELIVERY-PROCESSES WITH UML
Dr. William Goossen, Results 4 Care.
1. Introduction
To be able to support care with information systems the correct mapping of the care delivery-process to the system is essential. There are several ways to do this. In a project on perinatology it appeared that it’s good to begin with the information the care-professionals have: what patients do they have, what information do they need and what communication takes place. This can be combined with information collected from the domain of healthcare in general, for example national registrations, classifications and terminologies, guidelines and existing records. Care-professionals can be asked to order their activities chronologically and add comments about the practical situation the actions take place in. This is in order to get insight into the process. It’s important to have a complete understanding of the communication between care-professionals in information-analysis, the documents used and the information used. Work-processes (the handling of tasks by whom, on what moments and when), play an important role because they imply what information and documents need to be present at what time, in what form, to whom and with what purpose. This all has been explained in the first chapter.
After the analysis of a domain of care, the information modeling can take place. Modeling helps in communication with information technology experts and in the documentation of the electronic system. It might be necessary to visualize interactions between actor and system graphically. It might be beneficial to elucidate care delivery-processes. The graphic visualization with information modeling can be made using Unified Modeling Language (UML) (Booch, Rumbaugh & Jacobson, 1999). For the actors, communication processes and interactions in care delivery-processes the following diagrams are most important:
Use case diagram: describes which actors use the system Activity diagram: describes processes, sometimes the course of several processes in time Sequence diagram: describes the way care-professionals communicate Interaction diagram: describes how electronic messages are exchanged between systems.
Diagrams are essential for the designing of a complete system. In order to model the care-delivery-process after information-analysis several tools will be used. Some of them are discussed in the following text.
2. UML
The translation of a part of the care delivery-process into a model can be done with UML. UML (Unified Modeling Language) is an object-oriented modeling language with a mainly graphic method of registering. UML is standardized in 1997 by the Object Management Group. It has become the standard for object-oriented analysis and design. In healthcare several international standardization organizations, like HL7, CEN, OpenEHR and ISO, use UML to describe healthcare information models that are part of health informatics standards. In several cases reference models are being used. The HL7 Reference Information Model (RIM) by example is a special form of UML in which healthcare specific connotations are made. The HL7 RIM is widely used as a starting point for harmonization activities of several international standardizations. There are also alternative health care specific Reference Information Models, such as defined in the European standard series 13606 for health care. UML is the modeling method mostly used.
3. Business modeling
More and more information-systems are seen as an integrated part of management. Developing good information-systems demands thorough insight into processes they are part of, meaning the care delivery-processes. The aim of business modeling is not always the design of software-systems. It might also be used to gain a clear overview of the existing management. Besides this, it can be used to adjust the management or to redesign management-processes without needing to design a new information-system. When using UML for business modelling the assumption is made that there are parallels between the software-systems and the organizational system (business system). According to Booch et al (1999) several different graphical displays are used to portray the business. In our example the healthcare delivery-processes.
The different graphical displays are described here, seen from different perspectives:
• external functional perspective Use case diagram, with separate use cases the aim of the relation between actor and the business system are pinpointed. A use case describes the reason to use the system (e.g. care documentation in the EHR), the relevant actors and the major function of the system from the perspective of the user. Figure 1 illustrates the people that are involved with handling a request for a discharge assessment and the way this request is dealt with. • external interaction perspective Sequence diagram, the interactions between actor and business system are made explicit and ordered. In a way a sequence diagram describes a series of scenario’s (use cases). A sequence diagram is used to visualize the way two systems communicate electronically with each other. This is often also called an interaction diagram. The difference is mainly the way actors are being assigned, when in sequence in care professionals or organization, when with interaction-diagrams in information-systems like an EPF. People and organizations are involved in requesting family-care. The diagrams make clear what happens in the process and in what order. Dependencies are indicated in this diagram. The social worker can’t proceed as long as the information of this case is not complete. • internal process perspective Activity diagram, this tells us about the order of activities in time and the people/acts involved. It gives a simplified overview of what happens in a process. It shows the moments decisions have to be made. Figure 3 shows how this diagram can be used.
The following perspectives and their diagrams are not described in detail in this manual: • class diagram or object diagram, the description of company-entities and employees and important (clusters of) data (characteristics or attributes). Structural roles can be used. • internal resource perspective State diagram, per state the associated process in a system can be displayed.
The fact that one and only modeling-language is being used for business modeling as well as system-analysis and design offers many gains in communication and many possible ways of use of models (Van der Zee, 2000). For the drawing of the diagrams mentioned, special UML software can be used, e.g. Rational Rose, UML Studio, and Poseidon, or generic drawing programs like Microsoft Visio.
The diagrams as described here will be explained and practical examples will be given.
4. UML diagrams
As is mentioned before there are several UML diagrams that can be used to register activities and interactions between actors and the system. Certain diagrams play an important role for these activities and interactions in care-paths and care-chain. These important diagrams are illustrated with some practical examples in the following text. It often appears that by drawing models and discussing them with practitioners a new need for information evades, or things have to be readjusted, this is called an iteration: a method in which working forward to backward is alternated with working from backward to forward.
care-path, care-scenario or use case The care-path is a description of the practical care-situation. It is the basis for information-analysis and modelling. Care-path, care-scenario or use case can best be seen as synonymous with each other. Used methods in this step are interviews with care professionals, resource- and literature studies. Underneath is an example of a use case diagram.
Figure 1. Example of a Use-case diagram.
sequence diagrams These diagrams are often referred to as interaction diagrams. The use-cases are used as starting point and with the diagrams information about the process in the system are documented. The steps from the interaction from the use cases and the interaction diagrams are linked. The aspect of time is emphasized in sequence diagrams. The following guidelines are available in order to extract the correct number of sequence diagrams:
give every use case at least one sequence diagram; give any moment of choice in a use-case that gives direction for the continuation of the use-case one diagram for each direction; give, when there might appear great resemblance between diagrams, one diagram with connotations about the different events or series of events possible.
Figure 2. Example of a sequence diagram.
Plan of action for this type of diagram:
choose the use-case that has to be elaborated and from the different paths available the path that has to be elaborated; decide to which object the actor has to sent the message; elaborate if the object can answer the message directly; if yes, retrieve the answer, if no, determine what associated object is able to give the answer or which information is needed from other objects. Sent an event to these objects; repeat step 3 for all objects that receive an event; check if there are any restrictions in e.g. time or value and add these to the process; watch out for over-detailing when describing the interactions, it’s important not to loose the initial aim out of sight.
the activity diagram An activity diagram has great resemblance with a flow chart. It has some supplements though; the activity diagram shows steps, decision points and branching and joining. It can be used to illustrate the operations of an object and the processes of a company. In healthcare it’s a good tool to visualize who gives assignments, who receives them and what additional actions need to be executed and the way end-results are received by the principal. The activity diagram has its focus on the activities and the people involved. Every activity is represented as a rectangle with rounded edges. The symbols for the begin- and end-state are the large dots, massive for start and with a circle around it for the end. Decisions are represented with a diamond shaped form and with arrows indicating possible directions. It is possible to include feedback loops. Supplements are the so called ‘forks’ with which branches are depicted. In order to collect the paralleling processes ‘joints’ are being used as well.
Figure 3. Example of an activity diagram with swimming-lanes (HL7 Patient Care, courtesy of Isobel Frean).
5. Conclusion After the information analysis and the discussion and verification of the information with care professionals the models as mentioned are designed in order to describe the behavior of users in relation with the information system. The use case diagrams mainly describe the actors participating and the major function. The sequence or interaction diagrams describe the communication and the activity diagrams describe the way processes elapse. These models are often supplemented with extra models that aren’t described in this paper. From information analysis and modeling the next step can be to create a functional design, message specifications and an implementation manual. That is beyond the reach of this paper however.
Literature • Perinatologieproject (2002). Begrippenlijst Cd rom NICTIZ Modelleren. Leidschendam, Nictiz. • Van der Zee S (2000). Business modelling met UML. Software Release Magazine 3 Booch G, Rumbaugh J, Jacobson I (1999). The Unified Modeling Language User Guide. Boston etc., Addison Wesley.