This wiki has undergone a migration to Confluence found Here
2017-03-16 CIMI Telecom Minutes
Jump to navigation
Jump to search
<<< Pending Approval >>>
- 2017 Minutes: http://wiki.hl7.org/index.php?title=CIMI_Minutes
- Screen Sharing & Telecom Information: IHTSDO has generously provided a GoToMeeting connection for CIMI use.
- https://global.gotomeeting.com/join/754419973 Dialin: United States : +1 (224) 501-3316 Access Code: 754-419-973
- More phone numbers: Australia: +61 2 8355 1034, Belgium: +32 (0) 28 93 7002, Canada: +1 (647) 497-9372, Denmark: +45 89 88 03 61, Netherlands: +31 (0) 208 084 055, New Zealand: +64 4 974 7243, Spain: +34 932 20 0506, Sweden: +46 (0) 853 527 818, United Kingdom: +44 (0) 330 221 0098
- Telecom Audio: https://1drv.ms/u/s!AlkpZJej6nh_k7906pJl4wSDGh7sMg
- Telecom Video: http://www.opencem.org/cimi
- Co-Chairs: Stan Huff, Linda Bird, Galen Mulrooney, Richard Esmond; where, quorum requires 2 co-chairs
- REQUESTED ACTION: Directly edit this WIKI page or send your feedback to CIMI@lists.HL7.org with your comments, questions, suggested updates.
Attendees
Linda Bird, Bruce Bray, Linda Buhl, Joey Coyle, Gary Dickinson, John Donally, Richard Esmond, Bret Heale, Stan Huff, Steve Hufnagel, Mario Hyland, Mark Kramer, Patrick Langford, Joe Lamy, Jay Lyle, Chris Macintosh, Susan Matney, Chris Melo, Galen Mulrooney, Claude Nanjo, Brian Pech Craig Parker, Serafina Versaggi.
Highlighted names were in attendance.
Executive Summary
- Susan reported that Wound Assessment requirements are done
- Wound panel being presented at LOINC next week.
- SOLOR developers reviewing skin assessment terminology spreadsheet next Monday.
- Patrick reported OpenCIMI web-site CIMI-browser update to show mind-maps
- CIMI-browser can walk the model hierarchy and enter at any level
- Claude and Galen have been meeting for last three weeks. FHIM will be updated in March.
- Ballot submission plan
- Claude's focusing on modelling and BMM tooling; them, working on Style guide, Wound Archetypes, reconcile Jan 2017 Ballot comments.
- Stan working on marketing pitch next week,
- Action (Stan): Update spread sheet.
- Mar 26 - final May Ballot submission
- ACTION (Jay): Refined CIMI process for CIC
- Decision (Claude) - descope wiki page generation tool
- Status (Richard, Graham, Claude) BMM to FHIR profiles to be done after we submit
- Action (Richard) - Assemble final pieces for ballot
- Claude's bandwidth reduced at end of March
- Viet Nguyen, Stan, Graham discussed FHIR managing group negative comments
- Graham requested CIMI to review Argonauts profiles for vital-signs (attributes, terminology-binding and value-set bindings)to demonstrate CIMI value.
- Richard: Argonaut profiles are small, using coded text and enumerated values; but, not terminology.
- Mario - Argonauts 1.0 implementation guide are working against DSTU2; not, STU3. 90% of organizations are working against DSRU3. DSTU2 and STU3 value sets are different ... Argonauts seem to want to stay with old approach.
- Mark - US Core is Argonauts on STU3
- Claude - QI Core is being developed against STU3
- Stan - we are doing logical models, which focus on clinical content ... LOINC codes, devices. We are not committing to mappings; but, attributes and terminology and value-set bindings.
- Craig - we need to have a purpose ... maturity, validity
- Galen: V2, V3, CDA, MU variations in terminology and value sets. CIMI needs super-set value-set. We need to push for consistency at HL7.
- Claude: CIMI logical models lead to consistency as seen in QI Core and US Core.
- Galen: CIMI needs to support (Mario's) test driven development
- Stan's goal to move people to one profiles by ask why profiles are different. We express CIMI preferred model as a lever to move people together. We need to specify LOINC or SNOMED bindings and bring them back to the group for change current and/or future versions.
- we need a process, with a feedback to correct their models because resources are owned by appropriate workgroups.
- Stan - we are irrelevant without providing feedback to people doing the work and to us on the drivers, such as MU.
- Galen - non-clinical workgroups do not understand the consequences of their actions.
- Patrick: we need to define principles, so other workgroups can do it right the first-time-around.
- Richard: stay harmonized with CMI, CQS and CIMI
- Claude: we need to have discussions with WGs, such as Pharmacy and PC to get feedback and evangelize.
- Stan: Goal is to allocate time to review other profiles
- 1:16:00 APPROVED VOTE: Group launches an effort to review Argonauts profiles and invite interested stakeholders. Vitals is focus.
- Richard suggest other call to include others, such as Ken Kawamoto
- Linda suggested including TermInfo group (Rob Hausam POC)
- Susan stated we need to build CIMI models for the profiles (in parallel; but, informed by the Argonauts' profiles).
- Linda - CIMI looked at heart rate in the past.
- Stan - good to have some results by May for joint meetings.
- Galen - cautious about doing this in April and May ... need Vital Signs Archetypes before we can do terminology.
- Claude - good to do; but, too much to do currently.
- Action (Richard): one page SOW document (how) ... work after May. Draft out on listserve by end of weekend.
- Action (Susan): share previous vital signs document.
Minutes (Annotated Agenda)
- Scribe: Stan.Huff@imail.org
- Telecom Audio: https://1drv.ms/u/s!AlkpZJej6nh_k7906pJl4wSDGh7sMg
- REQUESTED ACTION: Update wiki directly or send suggested changes to Scribe or cimi@lists.hl7.org
- Bolded Items were discussed/annotated to the agenda
- Record this call
- Agenda review
- Review/Approval of March 2 minutes – Moved Galen, 2nd Richard. Approved
- Brief updates on active projects (standing item)
- Skin and wound assessments – Jay and Susan
- FHIM – CIMI integration – Galen
- Harmonization of CIMI and FHIR datatypes - Richard
- Graph/STAMP modeling paradigm – Richard
- Conversion of CIMI archetypes to FHIR logical models to FHIR profiles – Claude
- BMM parsing and serialization code – Claude
- Creating ADL models from CEMs – Joey
- LOKI – Patrick
- CIMI Website – Patrick
- Tool that takes the BMM patterns and produces FHIR profiles [Richard, Michael van der Zel]
- Ken Lord MDMI tool – Steve and Richard to follow up
- Help to create documentation tool that reads a model and generates wiki pages (a document generation tool) [Claude, Michael van der Zel]
- Review progress on the May ballot
- Work plan
- 3/26 publication date
- 3/1 full content draft
- 3/10 content done
- 3/14 docs done: to Patrick for editing
- Ballot content (top priorities)
- Modeling content [Claude, Galen, Jay, Susan]
- Documentation [Patrick, Editor]
- Need to make changes based on input from last ballot (Claude)
- Overall assembly of the ballot – Richard (with coaching from Claude)
- Overview/marketing pitch [Stan, Jay, Claude, Steve, Nona, Ask Laura]
- Plan to complete next week
- Updated and fleshed out style guide [Susan, Jay, Steve]
- Add content to Example spreadsheet (Stan)
- Architecture guide [Claude]
- Holding off until the architecture is more stable, then he will do a new version that incorporates all of the changes
- Refine CIMI Process Definition for CIC #3 [Steve, Claude, Jay, Galen]
- Jay will clean up and post to Google Docs for review next week
- Work plan
- Brief review of SWOT draft – Richard, All
- Those who have reviewed the SWOT thought it was a good starting place. People are welcome to suggest edits. We will plan to approve on the next call.
- Review of documents for the ballot submission - Claude
- Proposed review of FHIR profiles being created by other groups (i.e. Argonauts) – Stan
- Richard will make a proposal for how we would practically implement this intension.
- Review proposed changes to the model – Claude, Galen
- Review of updated assertion/evaluation table content - Stan
- Future topics
- Loading of concepts into SOLOR – Susan Matney
- Review CIMI Observation Result pattern - Stan
- How will CIMI coordinate with DAF? - Claude
- Granularity of models (schematic anchors) – from Richard
- We need a way to identify the focal concept in indivisible and group statements
- We would probably use the new metadata element
- New principle: Don’t include static knowledge such as terminology classifications in the model: class of drug, invasiveness of procedure, etc.
- Proposed policy that clusters are created in their own file – Joey, Stan
- The role of openEHR-like templating in CIMI’s processes - Stan
- IHTSDO work for binding SNOMED CT to FHIR resources – Linda, Harold
- Which openEHR archetypes should we consider converting to CIMI models?
- Transform of ICD-10 CM to CIMI models – Richard
- Others?
- Any other business
Annotated Figures
- Scribe: Stephen.Hufnagel.HL7@gmail.com
- Telecom Audio: https://1drv.ms/u/s!AlkpZJej6nh_k7906pJl4wSDGh7sMg
- REQUESTED ACTION: Directly edit this page or send suggested changes to scribe or cimi@lists.hl7.org

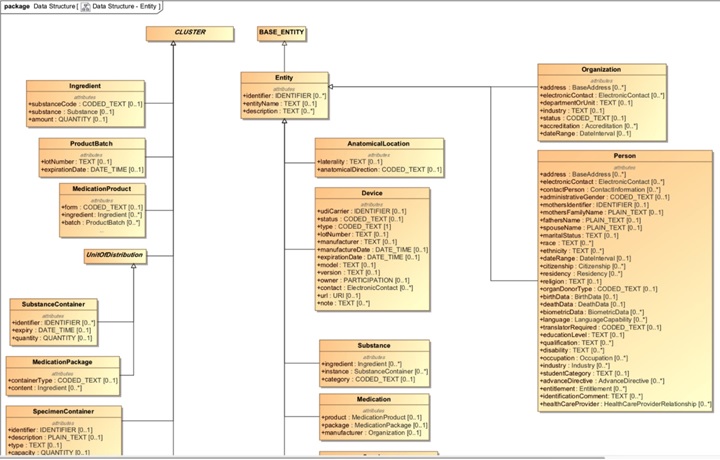
- Issue: Renamed material_Entity as Entity how can an entity be an actor? Some actors can-be non-human. Can’t use dual inheritance
- allowing entities to be actors gives more flexibility
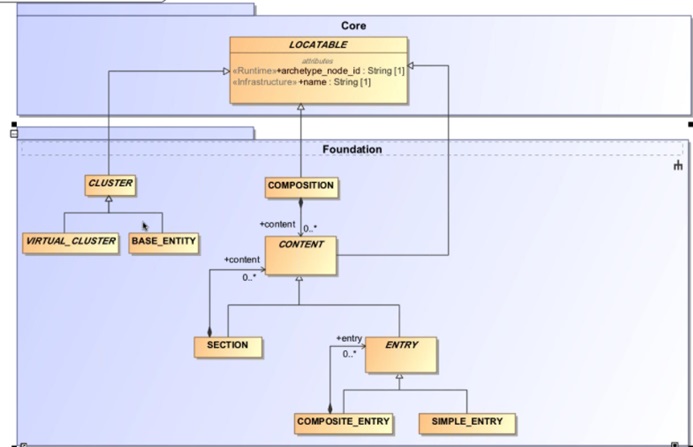
- need a Base_Entity in Foundation BMM
- ACTION (Richard): recommendations on Data Type changes

- ISSUE (Claude): any ENTITY can act as an ACTOR; such as SUBSTANCE in a bio-chemical process
- Specialization of CLUSTER as BASE_ENTITY; because, classes can’t have the same name across packages.
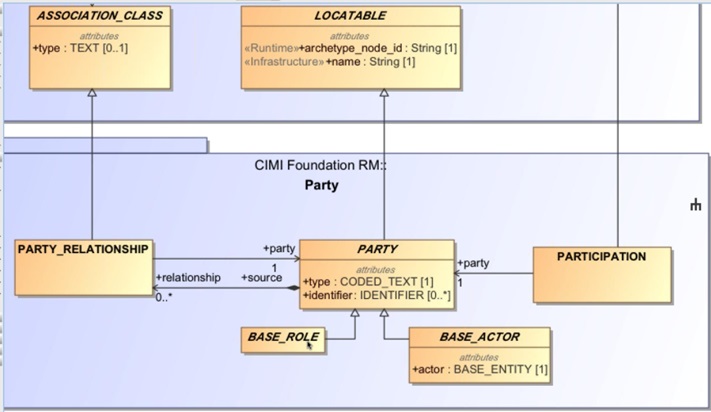
- ACTOR is a subset of BASE_ENTITY
- Party is defined by an Actor, which is an entity
- can be restricted at Architype level to be person or organization.
- PARTY has Role and Person specializations and Parties can be related to each other by Party_Relationship
- In Clinical model, rename MATERIAL_ENTITY as ENTITY to generalize and capture other things such as organizations
- Proposal: Actor references Person in organization by composition


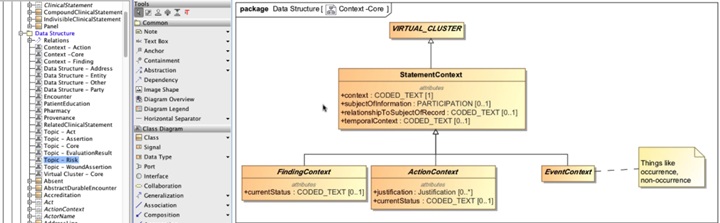
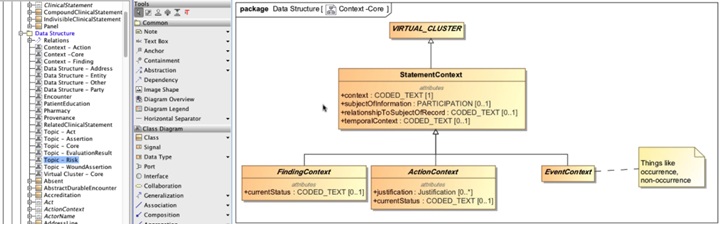
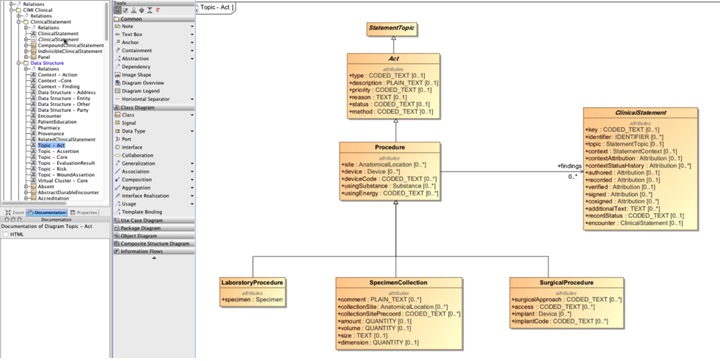
- Other Change: Statement-Topic-Context, Act planning or performed, etc.; but natural disaster event type things doesn’t work
- Event context might occurrence and non-occurrence third specialization
- SNOMED has-a event hierarchy, SNOMED has a due-to concept. Clinical finding is due-to an event (Linda)

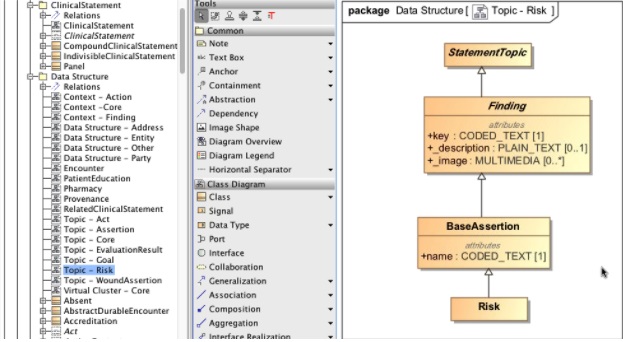
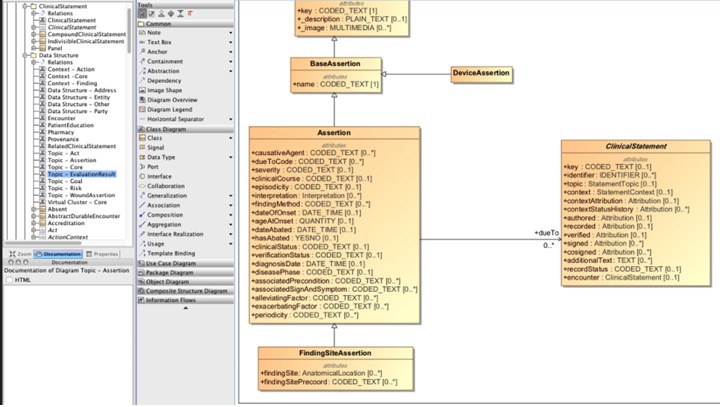
- Risk is present or absent a type of Assertion rather than a type of context.
- Stan: risk may be a sibling of Assertion rather than child. There are attributes of Risk like Assertion of Existence

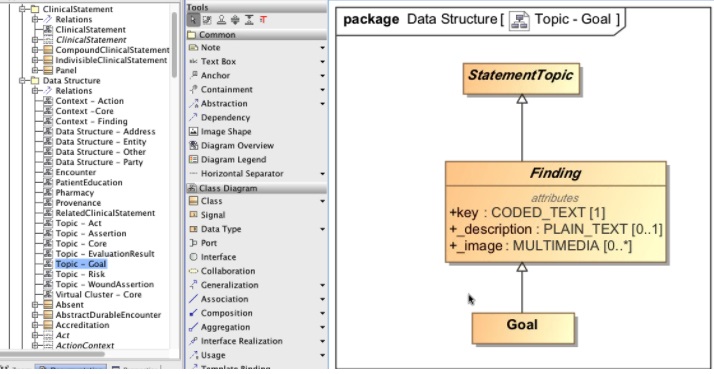
- Statement-Goal used to be a Context,
- Goal is a sibling of Assertion rather than a Finding
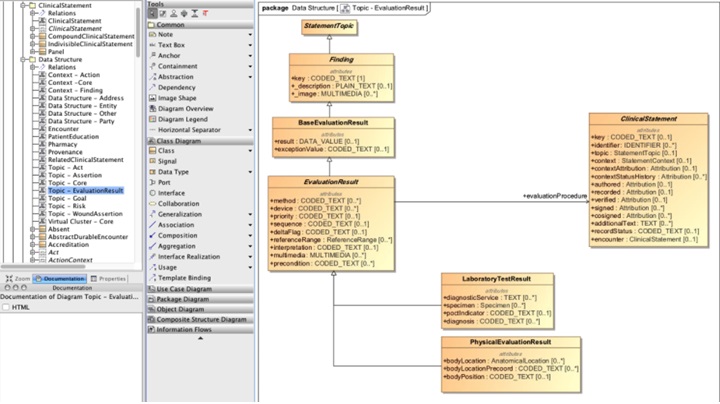
- Goal may be a subset of Base_Evaluation_Result
- Goal may also be a type of Base_Assertion
- Change to Statement-Goal with 1,* contexts
- Goal context may be similar to ActionContext with lifecycle states



- Goal context may be similar to ActionContext with lifecycle states



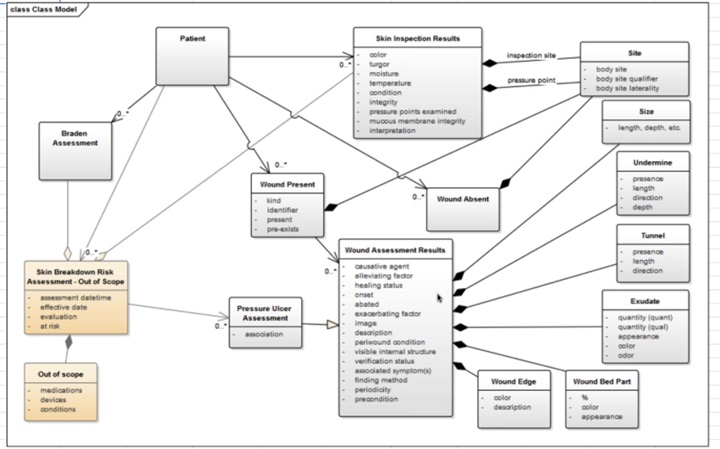
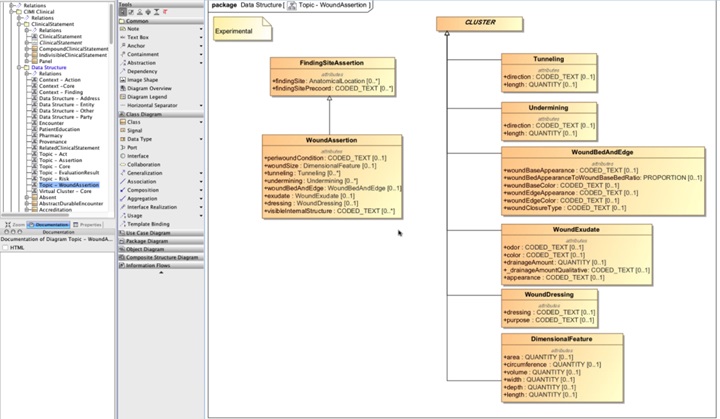
- Claude: (2:23:00) Do we need Wound Present or Wound Absent (Susan: No, can do Wound Assertion with Context of Absent)
- Claude: Skin Assessment Result modeled as panel, since we can have multiple wounds? Stan: Yes
- Claude: Interpretation applies to whole panel as another evaluation result? Stan: Yes and can be included in Panel.
- Stan: Panels can have shared provenance and shared attributes, such as blood pressure systolic and di-systolic BP.

- Skin inspection modeled as a panel

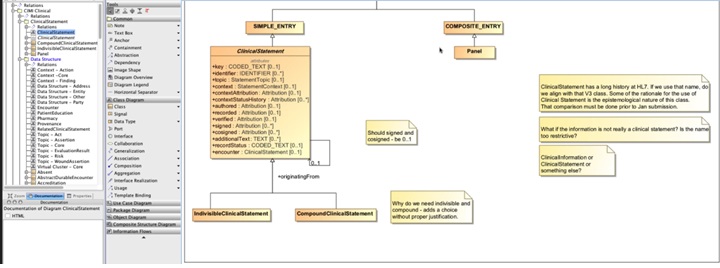
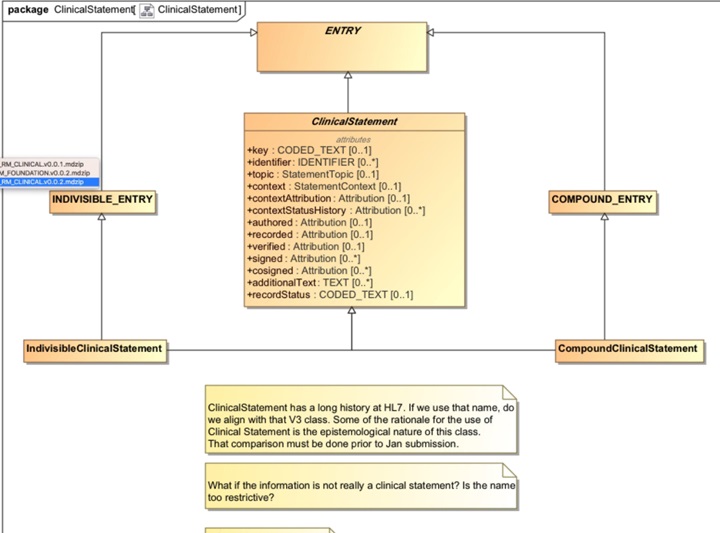
- Linda: Why is Panel a COMPOSIT_ENTRY rather than a CompoundClinicalStatement. Time-series of Observations.
- Historically, panel was a compoundClinicalStatement
- Panel does not Topic and Context and the entries can live by themselves
- Linda: rename ClinicalStatement to SimpleClinicalStatement and Panel have all the attributes of ClinicalStatement
- helps querying Panels vs ClinicalStatements; where, IndivisableClinicalStatement is the smallest meaningful units
- Linda – time series is a simple entry with multiple observations, such as a sensor for voltage or pressure
- Claude KNARTS branch of Composite and Simple Entries
- Linda – time series is a simple entry with multiple observations
- Linda – Can we model Section sub-types of ClinicalStatement or KNART ENTRY?
- Claude: No
- Linda: Can we have ENTRIES be recursive?

CIMI2017-03-02-16Package_ClinicalStatement.jpg
