This wiki has undergone a migration to Confluence found Here
RIMBAA 201101 Minutes Sydney
Revision as of 04:00, 13 January 2011 by Rene spronk (talk | contribs) (→(January 13th) THUR Q3 - Room 5.02 Image:Technical med.gif)
Agenda for the January 2011 WGM (January 9-14) in Sydney Australia
Contents
(January 13th) THUR Q3 - Room 5.02 
- Ren called to order at 13:45
- Administrative
- Announcements
- This quarter as well as the next quarter will focus on the commonalities between OpenEHR implementation issues and RIMBAA implementation issues. The focus will be on software development issues only. Modelling discussions as well as modelling tools are out of scope for this session.
- The agenda below was created based in consultation with OpenEHR implementers to ensure that we'd cover topics of interest to all attendees.
- Announcements
- Systems implementation guide for ISO 21090 (Grahame Grieve, max 20 minutes)
- Grahame: lots of centention, especially from Thomsa beale, about 21090. It'wasn't initially clear what the issue what.
- HL7 modeling expectation, when systems A and B communicate, is G: worst case, systems don't share anything. "offensive interoperability". refelcets day to day sitiution. It's not always like that, but have to make offensive case work. 21090 is "for exchange" worst case scenario. datapayse are build to be robust. We try to move away to 'best case scenario', one team sharing a library. Same teams, same boss. radically different environment. 21090 featuse to deal with offensive stuff start to be annoying in such an environment. OpenEHR towards 'best case" operability. Internat acrhitecture isn't set up to fail, nopt based on offensive principles. NCI has been told 21090 is ready for systems implementation. ICI also at deeplibraru sharing 'best case'scenario. Intent of 21090 wasn't to deal with 'best case'.
- Thomas Beale and Grahame have decided to create such a guide to mainly address the datatype denormalization issue.
- Will document the above issue, will present an alternative design, more focues on B P, transform away (basically two ways).
- Ex CD dt. Core concept itself, binding of code (orginal text text), plus capture of code (e.g. value set). Normalize out those 3 things out.
- Will provide a core UML model, XMI, a (maybe even MIF, if so requested by RIMBAA implementers, although MIF is probably too abstract).
- discussion: Sam: alligns with Intermountain work, they have defined requirements and have implemented. Grahame: requirements gathering will be problematic.
- Rene: model for interop, m for persistence? Grahame: I skirted that issue..
- Grahame: should be available before the Orlando WGM (May)
- Topic: persistence, based on reference model
- of Archetype/DCM/Template/SMIRF Instances
- using the reference model / RIM as a LDM
- See also (RIMBAA): Implementation aspects of RIM based database models, Temporal aspects of RIMBAA databases, ORM best practices
- Exchange implementation experiences. By its very nature OpenEHR covers this are in more details than HL7 ever could.
- Hugh: OpenEHR doesn't have a spec related to the persistence of models. Spec is however about a system, it defines the business layer of an EHR.
- Heath: EHR info mode, demographic inf mode
- ehro info mode, XML blob approach, initially SQL server, that was not efficient. Binary serialization of XML, improved storage and desirialization speed considerably. series of index tables, metadata about document/composition. Every RM attribute turned into rel table. Acrchetype Id / semantic signifiers in the blob, scehmatic of the thing that is contained in the blob. Approach succesful in patient vcentric scenarios, where the number of compositions within a single ehr is low, poplution scenariosn this gets a bit of an issue. Hugh: Minimum commmit is a [versioned] composition ('one or more archetypes').
- demographics: entry level (clinical statement level): store blobs at that level, extract certian bits of metadata. Decision is up to software developer what data to index (i.e. based on serach patterns).
- Other openWEHR implementatiosn are doing other things, e.g. using object databases, hibernate, ORM.
- Hugh: granularity is an issue.
- Rene .. on RIMBAA persistence object graphs table per class, table per hierarchy, OLAP, OLTP.
- Mark: looked at sevarl RIMBAA vendors, lloking at scalability, millions of patients, fas response time. Using ways of mapping ORM, 6 tables, metamodel driven processing. metadata for ORM mapping. all systems have an object middle tier.
- Heath: rules engine based oin compositions that are being commiteed, for des support, and idnexing, e.g. population querying
- Health: what's the scope of these SMIRFs? Lorraine: depends a bit on the context. We've seen solutions for CDA that cut things up at the entry level. Rene: jury is still out on tjis question, some regard the clinical statement model as a SMIRF, others just a part of a CMET.
- Topic: run-time use of model repositories
- See also (RIMBAA): persentation by AMS this week as contained in these minutes, Tuesday Q6 and the presentation by Andy Harris (point 4 in these minutes, slides 8/9 of [1]).
- Exchange implementation experiences.
- Topic: user interface generation based on (annotated) models
- See also (RIMBAA) User Interface for RIMBAA Applications
- See also (OpenEHR) UIs and openEHR data and Challenges in UI implementation
- based on Archetype/DCM/Template definitions
- based on data types
- Exchange implementation experiences.
- Topic: instance validation in a 2-layer model environment
- Exchange implementation experiences.
- Topic: Model Driven Engineering
- See also (RIMBAA): MIF based code generation
- Exchange implementation experiences.
- Topic: Query execution techniques.
- See also (RIMBAA): Safe querying of a RIM-based data model, Query Expression and Execution Technology.
- See also (OpenEHR): ArcheType Query language description.
- Exchange implementation experiences. By its very nature OpenEHR covers this are in much more detail (Heath Frankel to lead the discussion)
- Next steps
THUR Q4 - Room 5.02
- Continuation of the agenda from THUR Q3
FRI Q1 - Room 5.06 (09:00-10:30)
Wrap-up, methodology issues surfaced by RIMBAA implementations
- Administrative
- Announcements
- Planning a new out-of-cycle in November 2011 in London, and potentially one in June 2011 in Amsterdam.
- Discussion of Object identity, and role identity management in general
- New issue: RIM based LDAP Registries
- New issue: Persistence Models versus Interoperability Models
MON Q4 - Room 5.06 
| Workgroup | Date/Time | Location | Chair/Scribe |
|---|---|---|---|
| RIMBAA WG | 2011-01-10, 15:30-17:00 |
Sydney, AU | C/S: Rene Spronk |
| Informal meeting, not quorate. |
Attendance (Marked X)
| At | Name | Affiliation | Email Address |
|---|---|---|---|
| X | Andy Stechislin | GordonPoint, CA | andy.stechishin@gmail.com |
| X | Lorraine Constable | CA | lorraine@constable.ca |
| X | Rene Spronk | Ringholm, NL | rene.spronk@ringholm.com |
Minutes
- The meeting is not quorate. An informal meeting was held instead.
- Administrative agenda items
- Announcements
- Rene: I talked with I/C this morning (Q1) about the perceived overlap in mission, name and scope between Implementation/Conformance and RIMBAA. The scope of RIMBAA has widened from its focus on the RIM to the gathering of best practices about v3 software implementation in general.
- I/C wishes to keep its name, change its mission to 'exclude software development', and to 'include testing'.
- RIMBAA may wish to change its name to 'software development' (?), and change its scope to be about software implementation of all HL7 standards, not just HL7 v3 or the RIM.
- Andy: name should be SAMBAA or RAMBAA or something, to keep on using a cool name.
- (added after the meeting took place, and as such this doesn't form part of the official minutes of the meeting) This idea was presented to the Foundation & Technology steering division on Monday evening. It was presented as a FYI only, without a request for any action on the part of the SD. Feedback from those present is that it makes sense. Woody comments on a statement by Rene related to the scope of the Tooling committee: it is within its scope to create implementation oriented tooling, and it is in the tooling roadmap. Rene: Indeed; anyway, RIMBAA has in its mission to support the creation of such tools by third parties, and as such there is no overlap. Create draft/updated mission statements, agree in WG, foward informatively on the SD list for comments.
- ACTION Rene to craft a draft/updated mission statement, to use that as a basis for discussions within the WG, and to forward any outcome to the SD list as an FYI for comments.
- Rene: I talked with I/C this morning (Q1) about the perceived overlap in mission, name and scope between Implementation/Conformance and RIMBAA. The scope of RIMBAA has widened from its focus on the RIM to the gathering of best practices about v3 software implementation in general.
- Announcements
- Report from the Canada Health Infoway fall partnership conference held on November 15-17 2010.
- This meeting contains presentations on RIMBAA topics, as well as a v3 implementation tutorials. Lloyd McKenzie, Lorraine Constable and Andy Stechishin will be in attendance, and they'll provide feedback to RIMBAA.
- Andy/Lorraine: meeting was probably more abstract than what RIMBAA is interested in. More architectural in nature.
- Focus of partner meetings is increasingly towards implementers. May a RIMBAA session may be helpful. Andy will investigate whether this is an option.
- ACTION: Andy/Lorraine to send URLs of key presentations and snippets of text describing their contents.
- ACTION: Andy to follow up on MBT (software itself, and/or its architecture) and message instance editor.
- Report on new issues/insights brought forward that the RIMBAA meetings in London and Cambridge.
- This item was not discussed.
- User Interfaces - generation from Templates/DCMs, NHS CUI project
- SMIRF - SMall Isolated RIM Fragments
- Discussion of RIMBAA Issues
- See RIMBAA Issues
- The Migration from HL7 v2 to HL7 v3 issue was briefly discussed.
- Rene raised a new issue: the implementation of LDAP based registries (notably for providers) whilst using v3-mappable models. (See the RIM based LDAP Registries page, empty as of the point of this meeting)
- Meeting adjourned at 16:40
TUE Q6
| Workgroup | Date/Time | Location | Chair/Scribe |
|---|---|---|---|
| RIMBAA WG | 2011-01-11, 19:00-21:00 |
Sydney, AU | C/S: Rene Spronk |
Meeting Attendance
| At | Name | Affiliation | Email Address |
|---|---|---|---|
| X | Abdul Malik Shakir | COH, US | ashakir@coh.org |
| X | Gavin Morris | Kestral, AU | gavinm@kestral.com.au |
| X | Grahame Grieve | AU | grahameg@gmail.com |
| X | Ian Bull | ACT health, AU | ian.bull@act.gov.au |
| X | Jane Curry | HIS inc, CA | JaneCurry@healthinfostrategies.com |
| X | Lorraine Constable | CA | lorraine@constable.ca |
| X | Mike Rossman | KP, US | michael.k.rossman@kp.org |
| X | Patrick Loyd | GPI, CA | patrick.c.loyd@gmail.com |
| X | Rene Spronk | Ringholm, NL | rene.spronk@ringholm.com |
Minutes
- Rene calls to order at 19:13
- Administrative agenda items
- Approval of the minutes of the London meeting
- MOTION to approve the minutes of the London (November 2010) RIMBAA meeting as present on the HL7.org website (Lorraine/Patrick, 6-2-0 Y/Abst/no)
- Announcements
- Rene briefly provides an overview of the agenda for Thursday which has been finalized earlier today.
- Planning of next meetings
- RIMBAA 201103 Agenda in Washington DC, USA
- Andy will inform HIAL in Canada about this meeting.
- RIMBAA 201105 Agenda in Orlando FL, USA
- HL7 UK has offered to host another RIMBAA meeting, to be held in November 2011.
- RIMBAA 201103 Agenda in Washington DC, USA
- Approval of the minutes of the London meeting
- Dealing with "Context" of a payload
- Rene: During the London UK meeting is was noted that various projects use similar approaches when it comes to dealing with the context of 'payload data'. The Canadian specs use subject and author in the ControlAct wrapper (only); Lorraine presented the fact that NCI uses v3 based services where subject and author are part of the service parameters and not the service payload, and RIMBAA has been discussing the concept of Context SMIRFs. These are all similar approaches to remove context from the actual payload.
- Patrick: in the pan-canadian message specifications, we needed more information (e.g. author, subject, but on occasion also information about key payload acts) in the controlAct wrapper for orchestration/business logic/security reasons, without having to look at the payload. This means we have defined more wrappers than those that are present in the UV specification; there are more variations depending on what set of 'context' needs to be exposed in the wrapper. Examples: patient specific wwrapper, non-patient specific wrapper, administrative/financial wrappers.
- Patrick: The motivation is purely for implementation reasons.
- Jane: allows for the checking of the validity of the author and the patient, helps with indexing of the information, and lowers the computational cost of processing.
- patrick: there is also a governance aspect in that having this typr of information in the wrapper is a harmonization aspect for model usage, it forces all users of the specifications to implement these aspects in the same fashion.
- Lorraine: at NCI we're bring this type of context data up to the Service control level, out of the payload
- Abdul Malik: is there a finite list of things that could be brought up to that context level?
- Patrick: it is a finite list. there are a number of pattersn, determined by what one needs to orchestrate about. We may be able to categorize business functions.
- Grahame leads the discussion into the aspect of context conduction. If you move the context elsewhere, you'll have to conduct it somehow when persisting the data (see Context Conduction in RIMBAA Applications). Grahame: every developer will have to tame that beast one way or another. The Instance Editor tool uses a longhand approach, blow it out.
- Grahame: there is an issue here that MnM hasn't touched upon and that is that HL7 doesn't publish persistence models. A payload R-MIM could state that Author has a 0..1 cardinality, but when you persist an instance there may very well be multiple authors because of authors inherited from the context of that payload R-MIM. Only very few people actually realise that this happens. If RIMBAA wishes to surface this issue it will have to take it up (ultimately) with MnM.
- ACTION Rene to create an issue page on the topic of Persistence Models versus Interoperability Models (empty as of the time of this meeting), and to put this on the agenda of a future RIMBAA meeting for further discussion.
- Creation of an LDM/PDM based on the RIM (Abdul-Malik Shakir)
- Rene: AMS was one of the first persons in HL7 to discuss a method for the creation of PDMs based on DIMs. He has been involved in such projects a number of times.
- AMS: the basics steps are:
- Determine which part of the RIM is in scope for the project. In most projects the model is not the entire RIM.
- Deal with datatypes .. in general, creation of 3rd normal form. Problem are the abstract datatypes (e.g. ANY). Collections are also an issue.
- AMS: The initial projects I was involved in (about 12 years ago) at CDC and LA County were all about collecting data; not about querying that data. I looked at the requirements and went "Looks like the RIM to me".
- The next project thereafter was about the creation of a (California-) statewide Immunization Registry, populated by HL7 v2 messages. "Looks like the RIM to me".
- Currently working at City of Hope (COH), where they have separate systems for each kind of disease. Not very efficient, in the process of creating a common 'disease repository'. "Looks like the RIM to me".
- Next to that creating a Social services related system in San Francisco, where they are using the 'Microsoft Entity Framework' instead of Hibernate as a ORM solution.
- Rene: What are the lessons learned form all of these project?
- AMS: the lessons learned are twofold:
- Don't tie yourself to the RIM, be practical, and use deviations if the situation calls for it. Example: Observations on an Entity (Examples: "age of the house", "person has a tattoo").
- The use of the Place to capture addresses was found to be very useful, regardless of how it ahs been modelled in the RIM. Captures more about locations than just the address.
- AMS: the lessons learned are twofold:
- AMS: I noted that my approach is different from that of most RIMBAA implementers we've seen up to now: I create a RIM-based database model, and use a RIM-agnostic business-object layer based on the analysis model. (NOTE: RP and AO cells in the technology matrix). Most other implementations focus on a RIM-based business-object layer and persist it using ORM in a RIM based database (NOTE: RO-RP).
- Use of a (meta-)model registry in a RIMBAA environment (Abdul-Malik Shakir)
- AMS: the latest version of the metamodel, as used in CoH is as follows. Most of this is based on prior cross-industry work, as such there's nothing new about this.
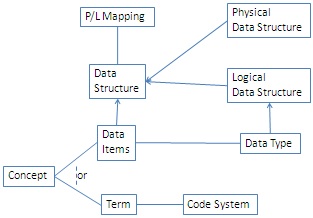
- AMS: a description of the model is as follows:
- When it comes to Data Structures we have two categories: Physical Data Structures and Logical Data Structures. Examples of Physical data Structures include a 'table with columns' or a 'form'. these structures can be valued. On the other han d we have Logical Data Structures. These are abstract specification models, e.g. the RIM.
- A Data Item may correspond to a Data Type; a Data Type itself is a Logical Data Structure. A Concept can be expressed as a Data Item or a Term, and Term is derived from a Code System (actually that part of the model contains value sets etcetera, we're focusing on the highlights).
- The P/L Mapping specifies the mapping from the Physical Data Structure to the Logical Data Structure and/or vice versa.
- The use case for CoH was to provide a "help capability", e.g. to get field definitions
- Meeting adjourned at 20:53

{kind=link}
Meeting Attendance (marked P)
| At | Name | Affiliation | Email Address |
|---|---|---|---|
| Abdul Malik Shakir | COH, US | ashakir@coh.org | |
| Adel Ghlamallah | CIHI, CA | aghlamallah@infoway.ca | |
| Alan Nicol | Informatics, UK | alan.nicol@informatics.co.uk | |
| Alejandro Pica | EMA, UK | alejandro.pica@ema.europa.eu | |
| Alexander Henket | E-Novation, NL | alexander.henket@enovation.nl | |
| Alex de Jong | Siemens, US | alex.dejong@siemens.com | |
| Alex Zupan | ItalTBS, IT | alex.zupan@italtbs.com | |
| Ameet Pathak | Dana-Farber Cancer Institute, US | ameet_pathak@dfci.harvard.edu | |
| Amnon Shabo | IBM, IL | shabo@il.ibm.com | |
| Andrew McIntyre | Medical Objects, AU | andrew@medical-objects.com.au | |
| Andy Stechislin | GordonPoint, CA | andy.stechishin@gmail.com | |
| Anil Luthra | Guidewire Architecture, US | aluthra@guidewirearchitecture.com | |
| Ann Wrightson | NHS Wales, UK | ann.wrightson@wales.nhs.uk | |
| Bill Friggic | Sanofi Aventis, US | william.friggic@sanofi-aventis.com | |
| Brian Pech | KP, US | brian.pech@kp.org | |
| Bruce McKinnon | JassCo, CA | bruce.mckinnon@jassco.ca | |
| Charlie McCay | Ramsey, UK | charlie@ramseysystems.com | |
| Chirag Bhatt | FEI Systems, US | chirag.bhatt@feisystems.com | |
| Chris Winters | Vocollect Healthcare Systems, Inc., US | cwinters@healthcare.vocollect.com | |
| Dave Barnet | NHS, UK | david.barnet@nhs.net | |
| David Rowed | Ocean Informatics, AU | david.rowed@oceaninformatics.com | |
| Diane Gutiw | SAIC, US | gutiwd@saic.com | |
| Duana Bender | Mohawk College, CA | duane.bender@mohawkcollege.ca | |
| Ed Larsen | Larsen Inc., US | e.laresen@ix.netcom.com | |
| Ernst de Bel | UMCN, NL | e.debel@ic.umcn.nl | |
| Ewout Kramer | Furore, NL | e.kramer@furore.com | |
| Gavin Morris | Kestral, AU | gavinm@kestral.com.au | |
| Gordon Raup | Carefacts, US | graup@carefacts.com | |
| Grahame Grieve | AU | grahameg@gmail.com | |
| Hugh Glover | BlueWave Informatics, UK | hugh_glover@bluewaveinformatics.co.uk | |
| Ian Bull | ACT health, AU | ian.bull@act.gov.au | |
| Ilia Fortunov | Microsoft, US | iliaf@microsoft.com | |
| Jane Curry | HIS inc, CA | JaneCurry@healthinfostrategies.com | |
| John Finbraaten | Marshfield Clinic, US | finbraaten.john@marshfieldclinic.org | |
| John Harvey | Iatric, US | john.harvey@iatric.com | |
| John Koisch | Guidewire Architecture, CA | jkoisch@guidewirearchitecture.com | |
| John Timm | IBM, US | johntimm@us.ibm.com | |
| John Ulmer | ??, US | johnu@clemson.edu | |
| Kai Heitmann | Heitmann Consulting, DE | hl7@kheitmann.de | |
| Kenneth Weng | CareFx, US | kweng@carefx.com | |
| Lyssa Neel | Infoway, CA | pneel@infoway.ca | |
| Lorraine Constable | CA | lorraine@constable.ca | |
| Marilyn Maguire | Fuji Med, US | marilyn.maguire@fujimed.com | |
| Mario Roy | Iatric, US | mario.roy@iatric.com | |
| Mark Bevivino | Iatric, US | markb@iatric.com | |
| Mark Shafarman | Shafarman Consulting, US | mark.shafarman@earthlink.net | |
| Mark Tucker | Regenstrief, US | mtucker@regenstrief.org | |
| Massimo Frossi | Ital TBS, IT | massimo.frossi@italtbs.com | |
| Michael van der Zel | Groningen University Hospital, and Results4Care, NL |
m.van.der.zel@ict.umcg.nl | |
| Mike Rossman | KP, US | michael.k.rossman@kp.org | |
| Muhammad Afzal | SEECS, PK | muhammad.afzal@seecs.edu.pk | |
| Patrick Loyd | GPI, CA | patrick.c.loyd@gmail.com | |
| Paul Boyes | Guidewire Architecture, CA | pboyes@guidewirearchitecture.com | |
| Peter Hendler | KP, US | peter@hendler.net | |
| X | Rene Spronk | Ringholm, NL | rene.spronk@ringholm.com |
| Richard Kronstad | Carefacts | rkronstad@carefacts.com | |
| Rik Smithies | NHS, UK | rik@nprogram.co.uk | |
| Robert Worden | Charteris, US | robert.worden@charteris.com | |
| Sean Muir | VA, US | sean.muir@va.gov | |
| Scott Parkey | Axolotl, US | sparkey@axolotl.com | |
| Stacy Berger | COH | sberger@coh.org | |
| Steve Fine | Cerner, US | sfine@cerner.com | |
| Tessa van Stijn | Nictiz, NL | stijn@nictiz.nl | |
| Tim Dodd | CA | tim.dodd@health.gov.sk.ca | |
| Tod Ryal | Cerner, US | tryal@cerner.com | |
| Yunwei Wang | Siemens, US | yunwei.wang@siemens.com | |
| Zhijing Liu | Siemens, US | zhijing.liu@siemens.com |